Sign up for the course! Click the ‘Register’ button below to register for the course. You will receive access to the full eight-module course.
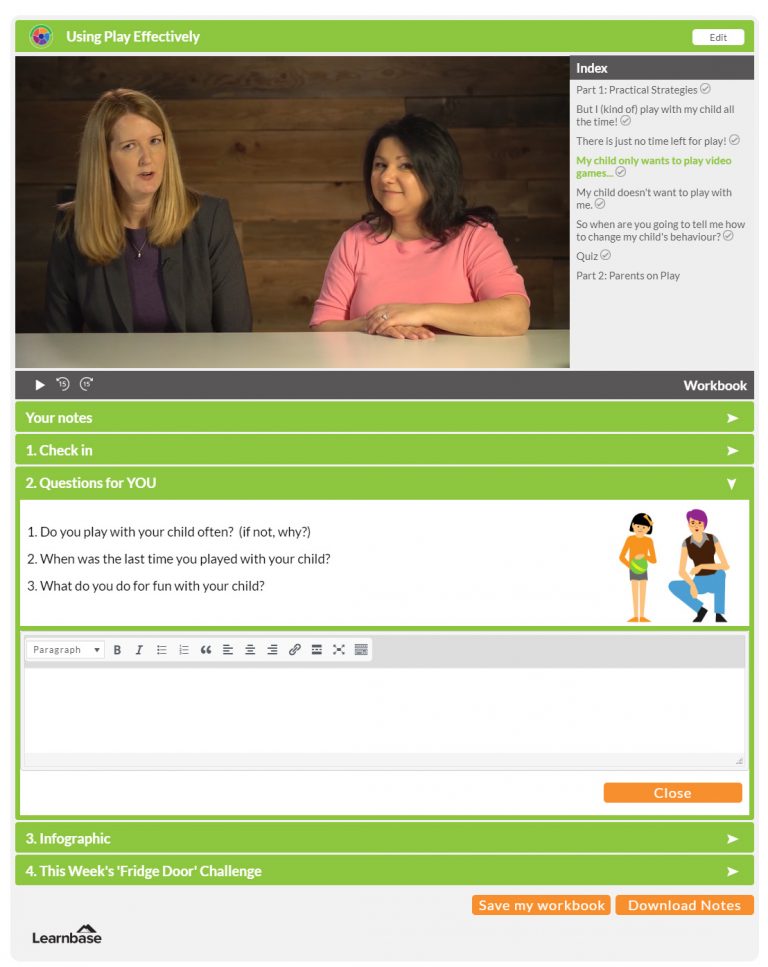
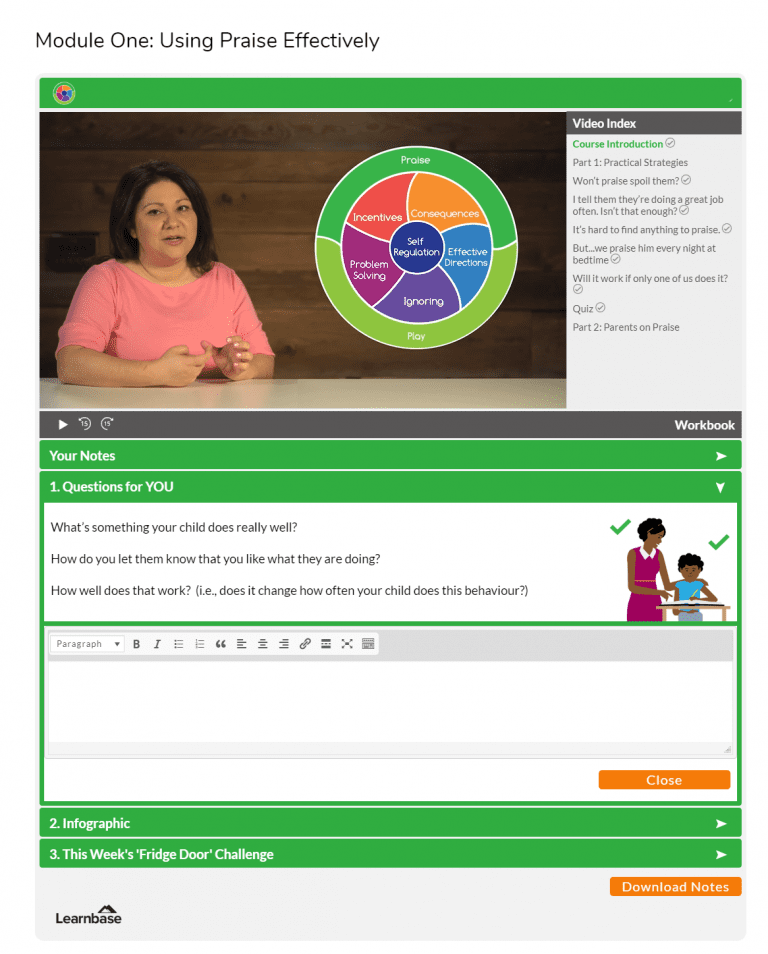
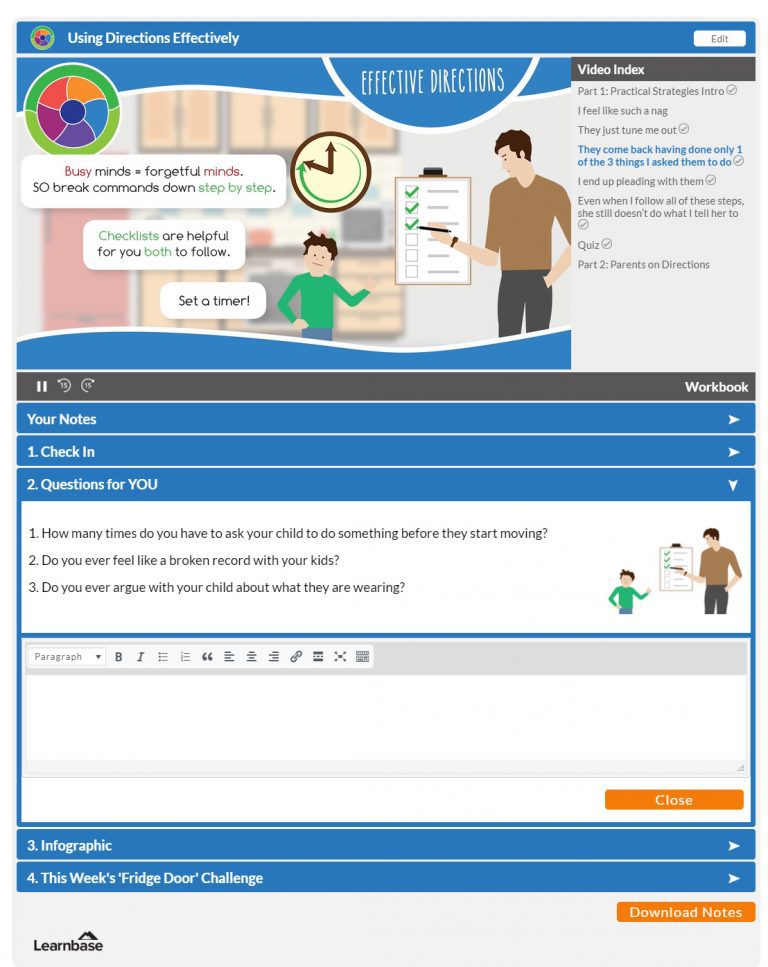
Short and impactful content – we know you’re busy! Each module includes a 15-20 minute video with activities to help you remember the key information and to think about how to apply the strategies to your family.
Focus on real life – You’ll be invited to reflect on how you have been approaching different issues with your children and how to start making adjustments.
Absolute Privacy – You’ll have a safe, secure space to interact as little or as much as you want with the course material.
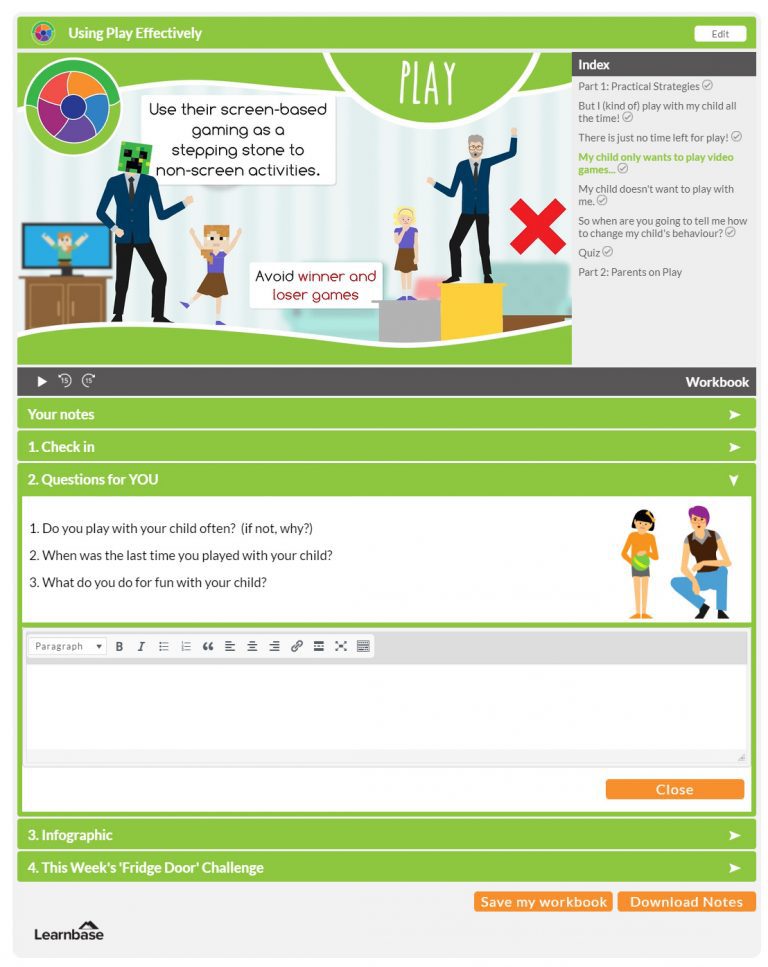
Our unique learning system allows you to create notes, make reflections and journal your progress in total privacy. The program also provides you with downloadable resources and a window into how other parents are approaching the everyday issues you face. You are not alone!