Rolling with ADHD for Parents
Module Four: Using Ignoring Effectively
✖
Using Ignoring Effectively
Video Index
Part 1: Practical Strategies
My child won’t know what’s going on. They will be really confused and frustrated.
The last time I was on the phone, my child kept asking me questions. When I didn’t respond, they just got louder and started following me around. Eventually, it turned into a big meltdown.
But I can’t ignore them when they’re running away in a parking lot.
I notice that he whines a lot when he gets home from school. It’s like a pattern.
It drives me bananas when she kicks the table at dinner. I can’t ignore it.
Quiz
Part 2: Parents on Ignoring
Your Notes
➤
➤
1. Check In
➤
➤
How well have you been able to apply some of the techniques from last week's 'Directions' class into your day-to-day? What impact have they had so far?
2. Questions for YOU
➤
➤
 1. What are some things your child does that annoys you?
1. What are some things your child does that annoys you?
2. What do you do about it?
3. Does it work?
3. Infographic
➤
➤

(Click image to download)
4. This Week's 'Fridge Door' Challenge
➤
➤
This week, we want you to choose one behaviour you want to change (e.g., tattling, interrupting), and one behaviour you can learn to accept (e.g., whistling, wiggling at the table) and practice ignoring them.
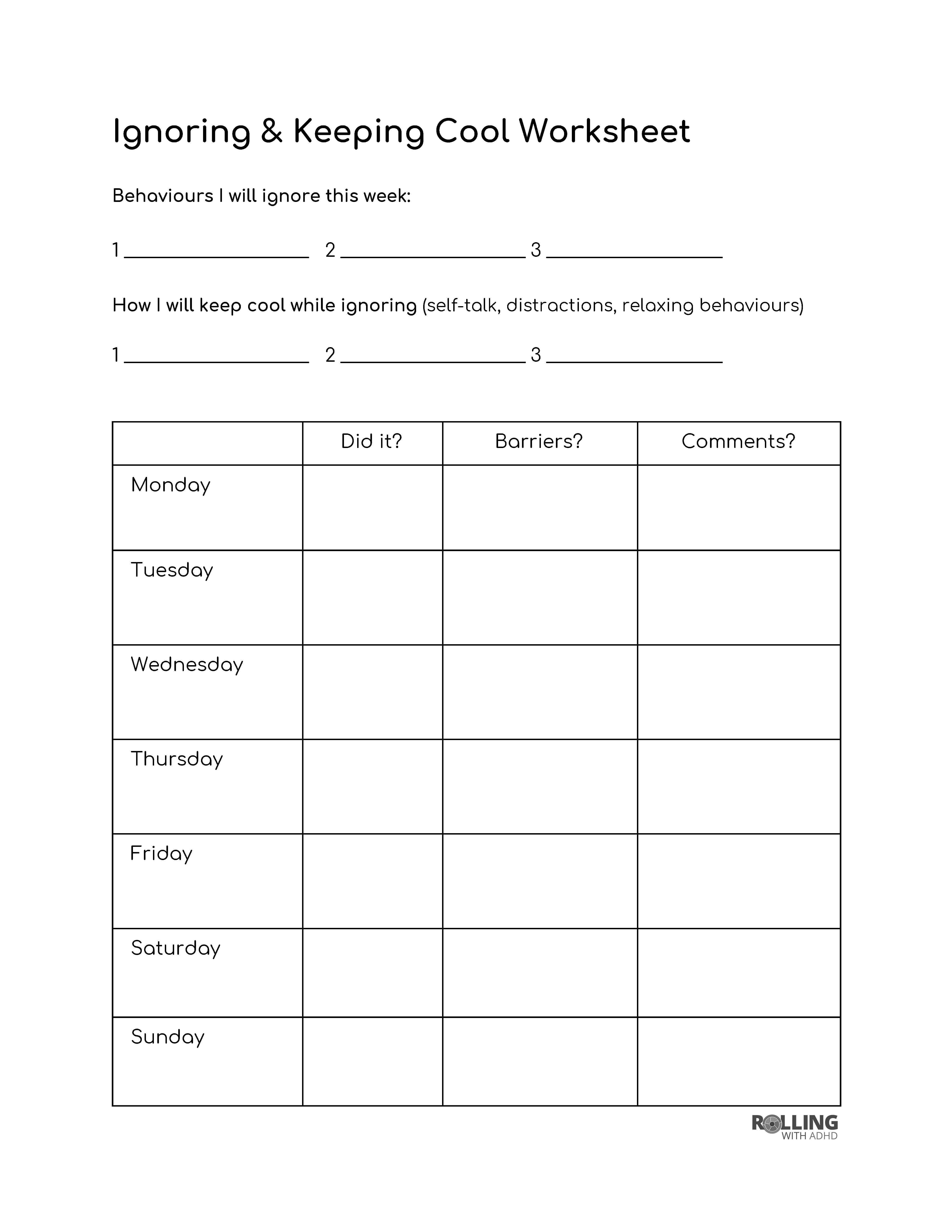
Keep track of how well it’s working with the tracking sheet provided. Click the image to download a blank version.
0%
Clear Notes