Rolling with ADHD for Parents
Module Five: Using Incentives Effectively
✖
Using Incentives Effectively
Video Index
Part 1: Practical Strategies
I told my child we could go to Disneyland if they got Bs on their report card. It didn’t work.
We tried using a chart. It worked for a while, but then stopped working.
How long do we have to do this for? It’s exhausting.
But I don't believe in bribing children.
Can I take points away for misbehaviour?
Quiz
Review Presentation
Your Notes
➤
➤
1. Check In
➤
➤
How well have you been able to apply some of the techniques from last week's 'Ignoring' class into your day-to-day? What impact have they had so far?
2. Questions for YOU
➤
➤
 1. Do you ever bribe your kids?
1. Do you ever bribe your kids?
2. Have you ever used a chart system and did it work?
3. How do you get your child to learn and use a new skill (like tidying their toys, making their bed)
3. Infographic
➤
➤
 (Click the image to download pdf version)
(Click the image to download pdf version)
4. This Week's 'Fridge Door' Challenge
➤
➤
Choose 1 or 2 behaviours you want to increase with incentives.
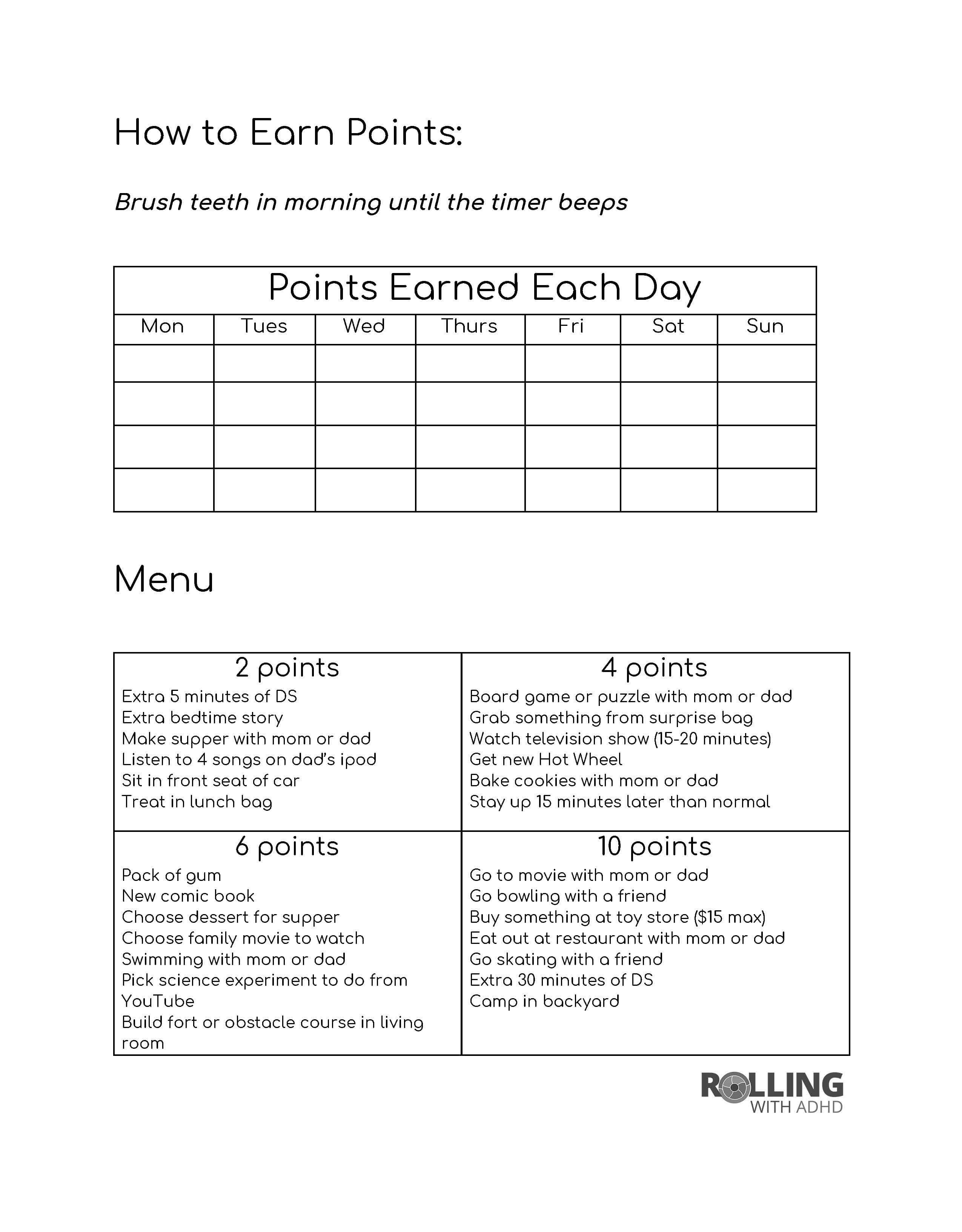
Use a tracking sheet like the example below to set up a reward menu with your child, and to track the behaviours.
Remember to set a day for your child to “cash in” on their reward and stick with it!
Click the image to download a blank version.
0%
Clear Notes